Portal Hypertension: Diagnosis, Management & Cure
Portal Hypertension : Portal Hypertension is among the most serious complications of advanced liver disease, particularly cirrhosis. When scar tissue forms in the liver, it obstructs the normal flow of blood through the portal venous system — the main vessel that carries blood from your digestive organs to your liver.
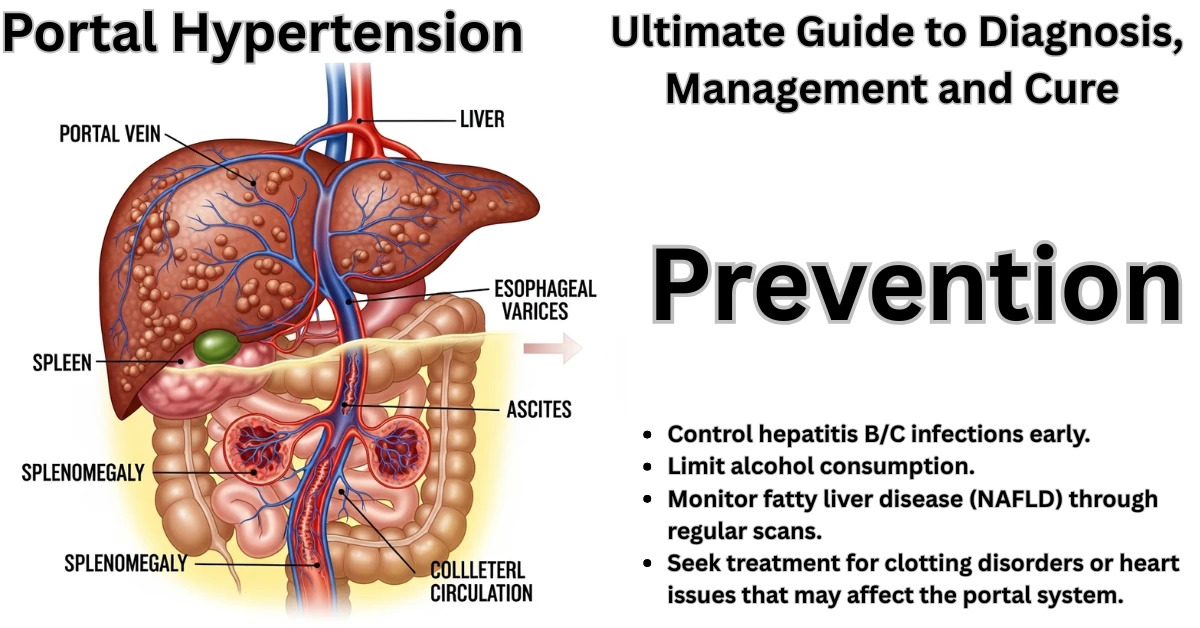
As a result, pressure builds up in this network, causing severe issues like esophageal varices, internal bleeding, ascites (abdominal fluid accumulation), and splenomegaly (enlarged spleen).
By 2025, advances in diagnostic imaging, endoscopic therapy, and minimally invasive procedures like TIPS have greatly improved the prognosis for patients with portal hypertension. Yet, it remains a condition requiring lifelong vigilance and expert medical care.
Let’s explore 10 powerful and proven insights about Portal Hypertension, its mechanisms, causes, warning signs, complications, diagnosis, and current treatment approaches that can truly save lives.
10 Powerful & Proven Insights on Portal Hypertension: Causes, Diagnosis, and Life-Saving Treatments
Table of Contents
🔹 1. What Exactly Is Portal Hypertension?
Portal Hypertension is defined as elevated blood pressure in the portal venous system, typically when the hepatic venous pressure gradient (HVPG) exceeds 5 mmHg. Clinical complications usually appear when it rises above 10–12 mmHg.
The portal venous system comprises veins from the stomach, spleen, pancreas, and intestines, which merge to form the portal vein, directing nutrient-rich blood into the liver for processing.
When the liver becomes scarred or obstructed, this blood flow is restricted. Consequently, pressure builds up and forces blood to find alternative pathways (collaterals), forming varices — fragile veins that are prone to rupture and cause massive bleeding.
🔹 2. Common and Rare Causes
Cirrhosis is responsible for nearly 85% of portal hypertension cases worldwide. However, many other causes exist and are classified according to where the blockage occurs.
A. Prehepatic Causes (Before Blood Reaches the Liver):
- Portal vein thrombosis (blood clot formation)
- Splenic vein thrombosis
- Congenital portal vein stenosis
- External compression by tumors or cysts
B. Intrahepatic Causes (Within the Liver):
- Cirrhosis (alcoholic, viral, or non-alcoholic steatohepatitis)
- Schistosomiasis (common in tropical regions)
- Primary biliary cholangitis
- Wilson’s disease and hemochromatosis
- Chronic viral hepatitis B or C
C. Posthepatic Causes (After the Liver):
- Budd–Chiari syndrome (obstruction of hepatic veins)
- Constrictive pericarditis
- Right-sided heart failure
Understanding the root cause is crucial because treatment strategies differ based on whether the obstruction is before, within, or after the liver.
🔹 3. Pathophysiology: How Portal Hypertension Develops
When liver cirrhosis sets in, the liver’s smooth architecture becomes distorted with fibrosis, nodules, and scar tissue. This fibrosis compresses the sinusoids (tiny blood channels), creating resistance to blood flow.
The body responds by:
- Increasing splanchnic blood flow (more blood coming from intestines)
- Developing collateral circulation to bypass resistance
- Releasing vasodilators like nitric oxide
While these compensatory mechanisms help in the short term, they eventually cause variceal formation, splenomegaly, and systemic circulatory dysfunction.
🔹 4. Early Signs and Symptoms
Portal Hypertension can remain silent in early stages. As it progresses, symptoms appear gradually:
General Symptoms
- Fatigue and weakness
- Loss of appetite
- Abdominal swelling and bloating
Visible Signs of Complications
- Ascites: Fluid accumulation in the abdomen
- Variceal bleeding: Vomiting blood or passing black stools
- Splenomegaly: Fullness in the left upper abdomen
- Spider angiomas on the skin
- Jaundice: Yellowing of skin and eyes
- Confusion or drowsiness: Due to hepatic encephalopathy
Recognizing these signs early can be life-saving, as complications can develop rapidly.
🔹 5. Major Complications of Portal Hypertension
Without timely management, portal hypertension leads to multiple severe complications:
A. Esophageal and Gastric Varices
These dilated veins in the food pipe or stomach can rupture suddenly, leading to life-threatening bleeding. Immediate hospitalization is essential.
B. Ascites
The most common manifestation. Excess fluid accumulates in the abdomen, often requiring paracentesis (fluid drainage).
C. Splenomegaly and Hypersplenism
An enlarged spleen traps platelets and blood cells, causing thrombocytopenia and anemia.
D. Hepatic Encephalopathy
Because toxins bypass the liver, they affect brain function—causing confusion, disorientation, or even coma.
E. Spontaneous Bacterial Peritonitis (SBP)
Infection in ascitic fluid—can be fatal if not treated promptly.
F. Portal Hypertensive Gastropathy
Chronic bleeding from fragile stomach vessels leads to anemia and fatigue.
🔹 6. Diagnosis: How Portal Hypertension Is Detected
Modern diagnostic tools have made early detection and grading of portal hypertension far more accurate.
Non-Invasive Methods
- Doppler Ultrasound: Measures blood flow and detects vein dilation.
- Transient Elastography (FibroScan): Estimates liver stiffness.
- CT or MRI Venography: Visualizes veins, varices, and liver structure.
Invasive and Endoscopic Tests
- Endoscopy: Detects esophageal or gastric varices.
- Hepatic Venous Pressure Gradient (HVPG): Gold standard for measuring portal pressure.
- Liver biopsy: Confirms cause (cirrhosis, fibrosis, etc.).
Doctors use these findings to stage the disease and plan individualized treatments.
🔹 7. Evidence-Based Treatments
Treatment depends on reducing portal pressure, preventing bleeding, and treating underlying liver damage.
A. Medical Management
- Non-selective beta-blockers (Propranolol, Nadolol): Reduce portal pressure.
- Nitrates: Enhance vasodilation and reduce resistance.
- Diuretics (Spironolactone, Furosemide): Manage ascites.
- Lactulose: Prevent hepatic encephalopathy.
- Antibiotics (Norfloxacin): Prevent SBP.
B. Endoscopic Management
- Endoscopic Variceal Ligation (EVL): Bands placed around varices to prevent rupture.
- Sclerotherapy: Chemical injection to collapse bleeding veins.
C. Radiological & Surgical Procedures
- TIPS (Transjugular Intrahepatic Portosystemic Shunt):
Creates an artificial channel between the portal and hepatic veins, lowering portal pressure effectively. - Surgical shunts: Reserved for non-cirrhotic causes or TIPS failure.
- Liver Transplantation: The definitive cure for end-stage liver disease.
🔹 8. Diet, Lifestyle, and Daily Management
Long-term survival depends not only on medical treatment but also on self-care and lifestyle adjustments.
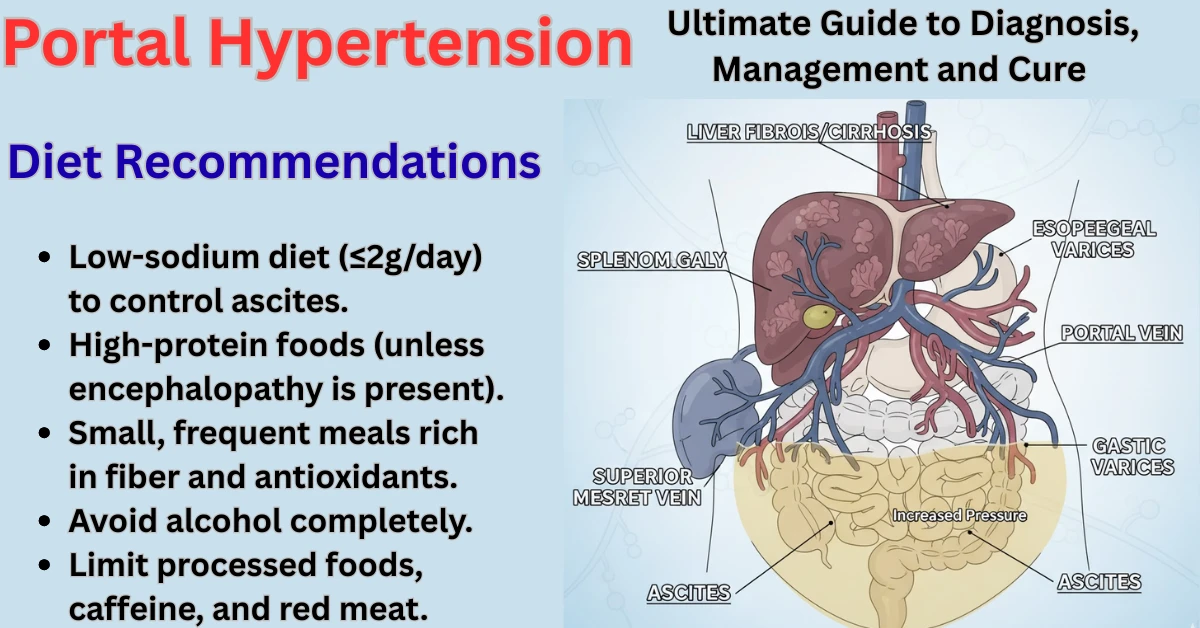
Diet Recommendations
- Low-sodium diet (≤2g/day) to control ascites.
- High-protein foods (unless encephalopathy is present).
- Small, frequent meals rich in fiber and antioxidants.
- Avoid alcohol completely.
- Limit processed foods, caffeine, and red meat.
Lifestyle Tips
- Maintain healthy body weight.
- Avoid unnecessary medications (especially NSAIDs).
- Get vaccinated against hepatitis A and B.
- Attend routine follow-ups and imaging every 6–12 months.
🔹 9. Prevention and Long-Term Prognosis
Prevention
- Control hepatitis B/C infections early.
- Limit alcohol consumption.
- Monitor fatty liver disease (NAFLD) through regular scans.
- Seek treatment for clotting disorders or heart issues that may affect the portal system.
Prognosis
The outcome depends on the cause and severity of liver damage.
With early diagnosis, beta-blocker therapy, TIPS, or transplantation, survival rates have improved dramatically.
Studies (2023–2025) show 5-year survival rates exceeding 70% with modern multidisciplinary care.
🔹 10. Emerging Treatments and Future Research (2025 Outlook)
Ongoing research aims to reduce portal pressure non-invasively and reverse fibrosis.
Promising Advances:
- Statins and Rifaximin: Shown to improve portal pressure by enhancing liver microcirculation.
- Antifibrotic drugs: Under trial to reduce liver scarring.
- Stem cell therapy: Potential to regenerate damaged liver tissue.
- Artificial liver support systems: Providing temporary relief before transplantation.
By 2025, these innovations are transforming portal hypertension from a fatal complication into a manageable chronic condition with the right care.
🧭 Conclusion: A Hopeful Outlook for Patients
Portal Hypertension, though serious, is no longer a death sentence.
With advances in medicine, imaging, and transplantation, patients now have access to effective treatments that dramatically improve life expectancy and quality of life.
Early diagnosis, strict lifestyle control, and consistent follow-ups remain the cornerstones of success.
Consulting a hepatologist and following a personalized care plan can truly make the difference between complications and recovery.
Also Read This : Revolutionary 24/7 Support: How CBSE’s Tele MANAS Partnership Transforms Student Mental Health
❓ FAQs on Portal Hypertension
1. Can portal hypertension reverse naturally?
It rarely reverses on its own, but early-stage hypertension can improve with lifestyle changes and effective treatment of the underlying cause.
2. How can I know if I have portal hypertension?
If you experience persistent bloating, vomiting blood, or jaundice, consult a liver specialist for imaging and endoscopic tests.
3. Is portal hypertension curable after liver transplant?
Yes. A successful liver transplant usually resolves portal hypertension completely.
4. What foods worsen portal hypertension?
High-salt foods, alcohol, fried items, and processed snacks worsen symptoms and fluid buildup.
5. Can portal hypertension occur without cirrhosis?
Yes, conditions like portal vein thrombosis or Budd–Chiari syndrome can cause it even in non-cirrhotic livers.
PortalHypertension #LiverHealth #Cirrhosis #Hepatology #LiverCare #Gastroenterology #HealthAwareness #MedicalEducation #PortalVein #LiverTransplant


